So says a Conservative minister in admitting that Andrew Lansley’s NHS reorganisation was the ‘biggest blunder of the Coalition government.’ I never thought I would admit it, but I think he is right. The Health Service is facing massive, and apparently intractable, problems, and many believe that the ‘reforms’ just made them all worse. Unsurprisingly, this view is prevalent within the medical profession:
Mark Porter, chairman of the British Medical Association’s governing council, said: “Rather than listening to the concerns of patients, the public and frontline staff who vigorously opposed the top-down reorganisation, politicians shamefully chose to stick their head in the sand and plough on regardless.
“The damage done to the NHS has been profound and intense, so this road to Damascus moment is too little too late and will be of no comfort to patients whose care has suffered.”
But, perhaps more surprisingly, this view is also found within the Government itself:
One insider said the plans, which were drawn up by Mr Lansley, were “unintelligible gobbledygook” and an ally of Chancellor George Osborne said: “George kicks himself for not having spotted it and stopped it. He had the opportunity then and he didn’t take it.”
A former No 10 adviser also told The Times: “No one apart from Lansley had a clue what he was really embarking on, certainly not the Prime Minister. He [Lansley] kept saying his grand plans had the backing of the medical establishment and we trusted him. In retrospect it was a mistake.”
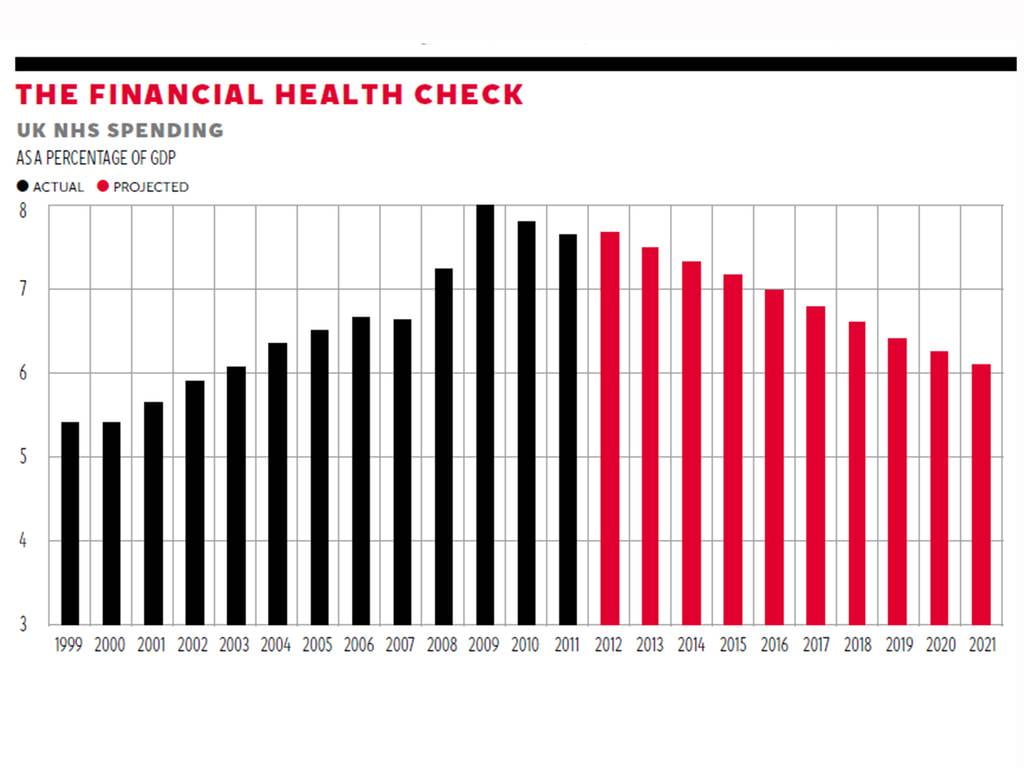 Despite this widespread opinion, the current Health Secretary, Jeremy Hunt, still defends the changes, and says they will deliver savings. In the discussion on Radio 4 yesterday morning, an external health analyst described the Government’s figures as being made up to get the answer that they were looking for, and just not reliable. You can see this when comparing past and future costs. Whereas past costs have risen relentlessly, somehow or other future costs are expected miraculously to fall.
Despite this widespread opinion, the current Health Secretary, Jeremy Hunt, still defends the changes, and says they will deliver savings. In the discussion on Radio 4 yesterday morning, an external health analyst described the Government’s figures as being made up to get the answer that they were looking for, and just not reliable. You can see this when comparing past and future costs. Whereas past costs have risen relentlessly, somehow or other future costs are expected miraculously to fall.
The most controversial part of the financial equation is the extension of PFI, the private finance initiative introduced by the Conservatives under John Major in 1992, but significantly expanded by Labour under Tony Blair. It is either the mechanism which is saving money, or a hidden financial drain on the NHS, depending on how you view it. In an open letter to politicians, Richard Laing, the General Surgical Registrar, highlights some alarming statistics about PFI.
The NHS will end up spending 80 billion pounds on hospitals that cost 11 billion to build (I believe one PFI hospital for example, will end up paying 4 billion pounds for their 380 million pound building). Most trusts that reside in a PFI building end up spending over 6% of their annual budget on PFI repayments and this can include extortionate maintenance costs.
The largest single player in the UK PFI market currently owns or co-owns 19 UK hospitals (and remarkably it only has 25 employees in stark contrast to the 1.7 million employed by the NHS). Their profit margin was 53 per cent in 2010 (apparently most successful FTSE 100 companies make margins of around 6 per cent). The founder and chief executive of this company, in 2010, owned almost three-quarters of the company (or 14 UK hospitals) and collected pay and dividends of £8.6 million, a significant proportion of which is essentially tax-payers’ money (I suppose that’s not very much when you consider it would only pay for the treatment of diabetes for just over five and a half hours, but still, it’s all relative).
One thing is not in dispute; as a result of the reforms, the acute care trusts within most of the healthcare regions are massively in debt, and there is a serious risk that organisations will start to fail.
It seems to me that there are three moral issues hidden amongst all these figures, one of which is rarely mentioned, and the other two never feature at all in the debate.
The first is the question of goodwill and the morale of health service employees. Laing points out that, contrary to most impressions, the NHS is remarkably efficient, in that it delivers a very good service at a much lower cost than comparable developed health care systems.
Health expenditure in the UK was 9% of GDP (USA 17%, Netherlands 12%, France 12%, Germany, Denmark and Canada 11%).
The UK had 2.8 physicians per 1000 population (4.0 in Germany, 3.9 in Italy, 3.8 in Spain, 3.3 in France, 3.3 in Australia).
The UK had 2.8 hospital beds per 1000 population (8.3 in Germany, 6.3 in France, 3.4 in Italy, 3.0 in Spain).
Average length of stay in the UK was 7 days (9.2 in Germany, 8.2 in New Zealand, 7.7 in Italy, 7.4 in Canada).
In comparison with the healthcare systems of ten other countries (USA, Canada, Australia, France, Germany, Netherlands, New Zealand, Norway, Sweden, and Switzerland) this year the NHS was found to be the most impressive overall by the Commonwealth Fund. It was rated as the best healthcare system in terms of efficiency, effective care, safe care, coordinated care, patient-centered care and cost-related problems.
And how does Laing account for this remarkable delivery? ‘It is because of the remarkable individuals who work for the NHS.’ All the more strange then that Lansley’s reforms were not based on the experience of those actually working in the system.
 The second issue is the NHS’s use of foreign medical expertise. Without drawing people to the UK to work in the healthcare system, the whole organisation would have collapsed long ago. Overall, 11% of NHS and community care employees were foreign nationals. But the figures climb steeply the more qualified you get. 14% of professionally qualified clinical staff are not British—and a staggering 26% of doctors. Nearly 10% of doctors come from a single country, India—and you do not need to think hard to work out which country (India or the UK) needs qualified doctors the most.
The second issue is the NHS’s use of foreign medical expertise. Without drawing people to the UK to work in the healthcare system, the whole organisation would have collapsed long ago. Overall, 11% of NHS and community care employees were foreign nationals. But the figures climb steeply the more qualified you get. 14% of professionally qualified clinical staff are not British—and a staggering 26% of doctors. Nearly 10% of doctors come from a single country, India—and you do not need to think hard to work out which country (India or the UK) needs qualified doctors the most.
This information rarely features in debates about immigration—but there is a further question to ask. How is it moral to suck this kind of professional expertise from other countries, simply because, for year upon year upon year, we have failed to train enough doctors and other trained staff for our own needs? This year the Midlands region has only been able to fill 63% of its training places for doctors.
The third moral question touches on the founding principle, and perhaps the most distinctive feature, of the NHS. ‘Free at the point of delivery’ is the untouchable mantra of all political comments about the health service. Woe betide any politician who suggests that this should change. But what is often forgotten is that this commitment was predicated on three assumptions about health and healthcare:
1. With the establishment of a free, national service, overall levels of health would improve.
2. The delivery of healthcare, after an initial step-change up, would not continue to become more expensive.
3. People would take more and more responsibility for their own health, so that in the long term, demand for care would fall.
In one sense, the first has come true, in that the overall health of the nation has improved drastically, with life expectancy continuing to rise. But the problem is that something like 80% of NHS costs relate to the last 10 years of life, and extending old age is just going to push costs up. The second is clearly false; one of the dilemmas in Western medicine is the availability of ever-more expensive forms of treatment, as shown by the controversy when cancer treatments are judged to be too expensive to make available through a ‘free at point of use’ system.
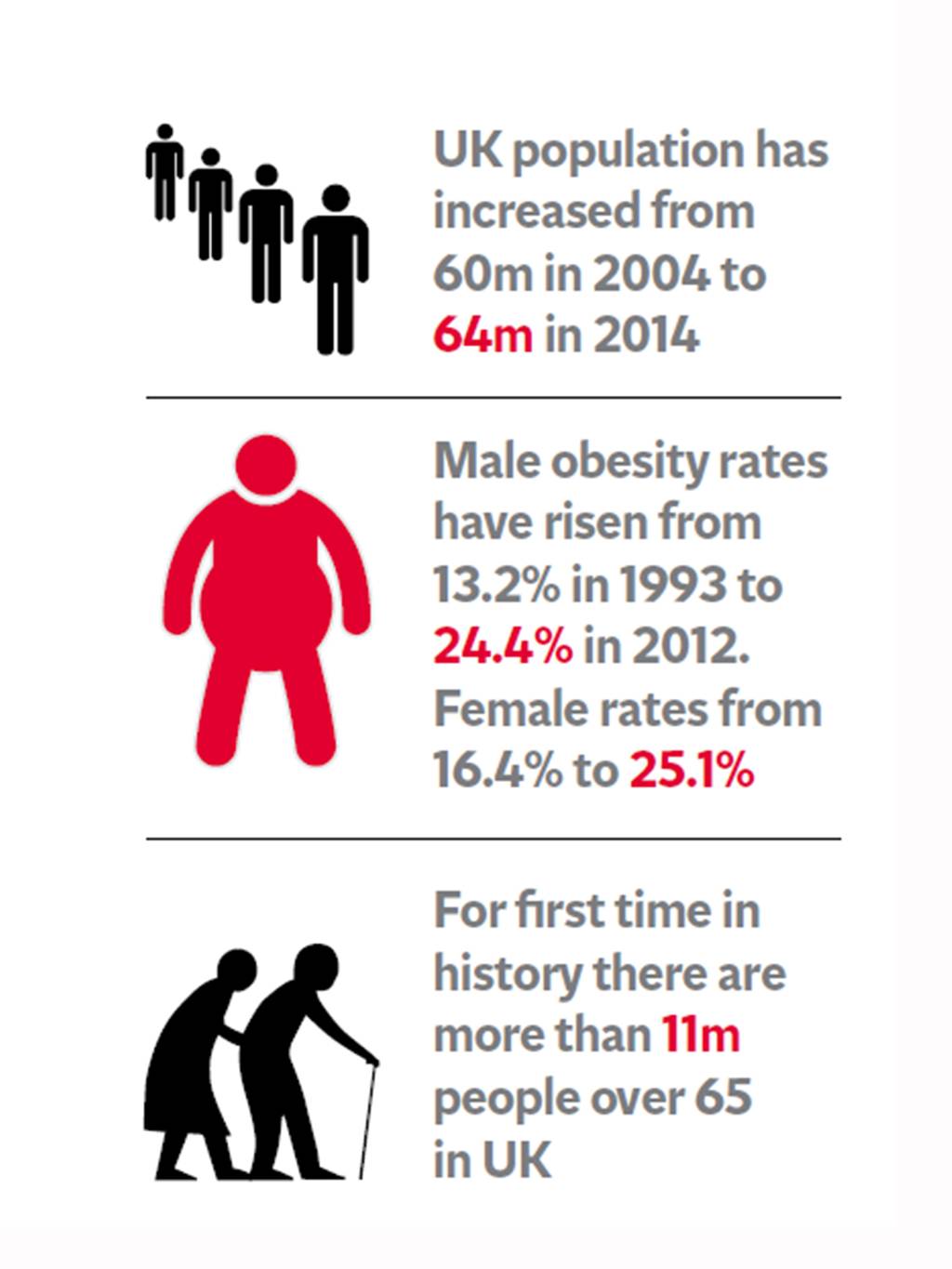 But the most challenging is the third. The two biggest strains on the NHS are obesity and alcohol misuse—entirely preventable issues under the control of patients. It is claimed today that 10 million hospital visits a year are due to alcohol misuse, leading to both acute and chronic illness. And obesity is increasing at alarming rates which will push up health costs and the demand on services. The moral dilemma comes from both sides. On the one hand, why should I proactively take care of my health when any problems that arise will be dealt with at no cost to myself? On the other, why should I continue to contribute to the healthcare of people who do not take responsibility for themselves when I do for myself?
But the most challenging is the third. The two biggest strains on the NHS are obesity and alcohol misuse—entirely preventable issues under the control of patients. It is claimed today that 10 million hospital visits a year are due to alcohol misuse, leading to both acute and chronic illness. And obesity is increasing at alarming rates which will push up health costs and the demand on services. The moral dilemma comes from both sides. On the one hand, why should I proactively take care of my health when any problems that arise will be dealt with at no cost to myself? On the other, why should I continue to contribute to the healthcare of people who do not take responsibility for themselves when I do for myself?
The issue here is a mismatch between a socialist, communitarian model of behaviour assumed in the ‘free at point of delivery’ commitment, and an individualist, free-market model of behaviour in the language of customers and service. The two cannot co-exist in a sustainable health service.
And yet this conflict is built into the basic processes of the NHS. The capitation system, where GPs are paid per patient regardless of how many times they visit, is based on the assumption that patients take responsibility for their own health. It creates incentives for doctors to encourage patients to do this—but it completely contradicts the idea that patients are ‘customers’ expecting to get a ‘service’, an idea made explicit by John Major with the ‘Patient’s Charter.’ Imagine customers in any other service context demanding a certain level of service when they have paid a fixed fee to get unlimited access to the product whenever they demand it. The system has created large disparities between wealthy areas, where patients visit less, and poorer areas with much higher levels of patient attendance. In the former, practices can take on more patients; the doctors there earn more; so jobs are easy to fill as there are many applicants per vacancy. In the latter, work is more demanding, doctors earn less, and practices find it hard to recruit.
Given these underlying problems, any political party trying to make the NHS work within budgetary constraints is attempting to square a circle. Even Lansley’s reforms are using private money to rearrange the deck chairs—though of course we might now enjoy a better quality of deck chair. We either need to abandon the individualist, market-led consumer model of patient behaviour—or start charging for the service at its point of use. There is no middle way.
Much of my work is done on a freelance basis. If you have valued this post, would you consider donating £1.20 a month to support the production of this blog?
 Buy me a Coffee
Buy me a Coffee












Is it morally unjust that Lansley and the civil servants responsible for this fiasco cannot be criminally prosecuted?
Indeed…and that is just what some have commented in the first linked article:
‘Experts said the reorganisation, which is estimated to have cost about £3bn, had caused “profound and intense” damage to the NHS with one saying former Health Secretary, Andrew Lansley, would be facing disciplinary action if he had been a doctor.’
and
‘Clare Gerada, who was chairwoman of the Royal College of GPs until 2013, said politicians and policymakers “need to have a long, hard look at themselves”.
“They are saying this now but they should have said it then. The big issue is that nobody has been held accountable for it. If Mr Lansley was a doctor, he would have been referred to the General Medical Council,” she said.’
You talk about obesity but this is the same government that allowed drink measures, bottles etc to get larger …. and you don’t want to throw half away. So governments are encouraging us to get obese and alcoholic (they are related).
I agree. It is odd that successive governments keep taxing tobacco, when this is now a much smaller factor in health. Some propose that there should be a tax on unhealthy food—but I guess that would be a regulatory nightmare.
It is bizarre that licensing laws have not been hauled back in.
There seems to be a conflict between the shortage of doctors coming through and the very high competition to enter doctor training. I don’t think it can be because there aren’t enough good applicants, but is presumably because there aren’t enough training places. A self-inflicted skills shortage.
V interesting points thank you Ian
a few thoughts:
1) Tax on Sugar could start help funding the cost of obesity ( and maybe raise the profile of the issue and start to help drive behaviours) no quick fix – but may help as part of the mix.
2) There are beginning to be prerequisites to certain procedures e.g. you can have this procedure once you have hit a weight target. I think this makes medical & financial sense and will inevitably be extended. Is there a way we can extend this to smoking, excessive drinking, etc… tricky to measure!
3) we will have to face up to the fact that decisions will have to be made on how much money we can spend on people based on age, health, lifestyle etc… Not a “nice” ( sorry bad pun) job but will become necessary as we live longer and more medicines are available, many at extreme financial cost.
4) It seems that the deckchairs are rearranged every time we change government – each change costs us £Bns yes this reorg was a complete failure but not that much worse than any others. I agree the biggest issue this time was probably the lack of consultation it is true!!!.
5) The lack of doctors crisis is a fundamental concern but probably even more acute in General Practice where demands are increasing dramatically but funding reaching them is reducing rapidly. This is not just a recruitment crisis – principles ( partners) are leaving in significant numbers.
It is important to remember that healthcare may be “free at the point of delivery”, but it is not free healthcare – after all, every wage earner pays contributions … so the title, “Free healthcare cannot continue” is somewhat misleading.
We have similar problems here in France, although no French government will ever dare introduce hated liberal market reforms into the health service.
Politicians talk of reform, but what they really mean is that they want the system to keep carrying on as it currently does, even though it’s impossible to fund adequately without raising taxes to punitive (or more punitive) levels.
What will happen here is what always happens. Politicians will write fine speeches about the wonder that is the French model of public service and while we’re all congratulating ourselves about how much better we are than those terrible money-grubbing English, the deficit will continue to grow until the point at which government finances will tumble into a big black hole and we’ll all go down with it.
Yes, the English ARE terrible money-grubbers. A nation of petit-bourgeois shopkeepers obsessed by profit and loss and bottom lines. But at least you understand that you have to live within your means. Over here we’re very grand and noble and have fixed ideas about liberty, equality, fraternity and free health care for all, but our governments have no more financial talent than Louis XVI and Marie-Antoinette. They think they can just spend their way out of trouble. And if they need more dosh, they’ll just squeeze us a bit harder.
They say history never repeats, but there’s a real stench of 1789 in the air at the moment. It’s like being in that wretched Delacroix painting with a bare-breasted Marianne (or Marine as she’s known today) leading a charge of assorted fascists, Catholics, skinheads and racists, all of them bent on destruction and revenge, while the president and his Spanish court jester sit in their palace doing strictement rien du tout about it.
You won’t have a revolution over there. You never do. But don’t be surprised if you wake up one morning to find a fascist government staring at you across la Manche. Or rather the announcement of a fascist government, quickly followed by the outbreak of revolution and civil war. That’ll sort your problems out for you. Britain is never so prosperous as when it’s fighting a war against one or other of its European neighbours.
Marine le Pen seems to be doing pretty well at the moment, so I would not be very surprised. Mind you, she says some surprisingly sensible things… She sliced and diced a Newsnight reporter a few months ago on the question of controlling immigration.
Ian,
I work for an architect’s practice and we’re currently working on a major PFI hospital project (Hiss! Boo!). I’ll admit some bias here, but let’s still look at the alternatives.
Instead of going for PFI, the government could just incur debt directly onto its balance sheet for those assets. Instead, we have a limited number of privately organized consortia capable of taking on the business risk of spiraling capital and operating costs over 30-odd years and hopefully making themselves a profit.
You can’t make that massive cost of shifting the risk disappear. It will hit public expenditure somewhere. In the case of the National Physical Laboratory, were it not for PFI, the over-spend would have had an even more severe impact on the public purse. As it was, the Joint Venture collapsed.
In the case of the Scottish Parliament, the traditional Design-Bid-Build procurement route had a catastrophic impact on their budget that could have been ameliorated by PFI.
The problem with restructuring is that the savings are long-range and strategic. What’s needed are more immediate tactics for reducing cost and improving service.
It does seem that the Department of Health has been unable to inspire enough morale to build the sort of lower-level leadership that would encourage and exchange ‘grass-roots’ best practices.
The focus is on an expensive top-down strategies that are supposed to deliver efficiencies at the ‘point of delivery’, but impose a greater workload on staff, especially junior doctors.
I wonder how much of the re-structuring involved genuine consultation with PCTs and GPs before implementation.
Free (at the point of delivery) healthcare probably cannot continue. The well-off will opt ever more for going private.
Nevertheless, whatever we end up paying, we only have to look across the pond and compare it with the Republican ‘am I my brother’s keeper?’ mindset. However much successive governments deface our NHS ideals and destroy staff morale, the relentless attempts to thwart Obama-care over there always seem a darn sight uglier.
But, David, the fact that companies involved in PFI are making such massive margins suggests that either
a. the Government is paying way too much, or
b. there is a good return to be made here.
I think either would suggest that, yes, Government would be better taking the cost of the assets onto their own books. It is political ideology, and not accounting, that has pushed them in the other direction.
WE forget that the NHS was run at first on cheap labour-students and trainees. At night in the 1950s in my London Training Hospital all wards were staffed by 2 student nurses and there was one Nursing Sister on each wing (about 200+ patients) Change was not expected “Once you’re trained . you’re trained”
.Changing health care, new treatments and research meant medical and nursing staff had to learn to do research in the pressure to keep up to date in practice.
Good care depends on good relationship between patients and cared, often made impossible by bureaucratic management systems- ;like the LEAN system developed by Toyato
I would change the culture which prevents relatives helping in the care of patients-especially in long-term care.
I would introduce the Primary Nurse model of care described in the Audit Report ‘The Virtue of Patients’ (and paid lip-service too by the authorities as ‘named nurses’)
I would like a good look at General Practice culture and purpose with patient representatives in management and more Nurse Practitioners taking a lead..
Jean, that is really interesting, thanks. What you are suggesting is another change in culture, though in a slightly different direction. It is odd that we are made to feel we have no responsibility for the care of relatives in hospital.
I live in the USA. Any time you get tired of your Health Care system you just send it over here and you can have ours — even trade.
No plans for that John!